Shamiri
Adolescence is tough, and there is little for kids to turn to when they need help.
The Idea
Peer-Led Youth Support Groups


Total Investment
975000
Grants
0
Equity/SAFE
0
Debt/Convertible Debt
Funded Since
2022
Geography
Sector
Structure
The Mission
Thriving young people.
How It Works
Shamiri's school-based, group intervention is delivered by recent high school graduates ("fellows"), who are trained and managed by supervisors. Fellows deliver a weekly one-hour class over four weeks, focused on gratitude and growth mindset to groups of fifteen students. All students participate and complete take-home assignments in between. Kids with serious mental health problems get referred to professional help.
The Dream
The Shamiri model is integrated into public high school curriculum.
Why We're In
Shamiri is part of a growing movement to test low-cost models to meet the need for mental health in Africa. Their approach centers on mental well-being for poor adolescents. The results are impressive: symptoms of depression and anxiety reduced by 38% and 45% respectively, even after a 7-month follow-up, and they’re testing government delivery and AI tools to make the model scalable. It’s a bet worth taking as they explore the link between better mental health and school outcomes.
Delivery
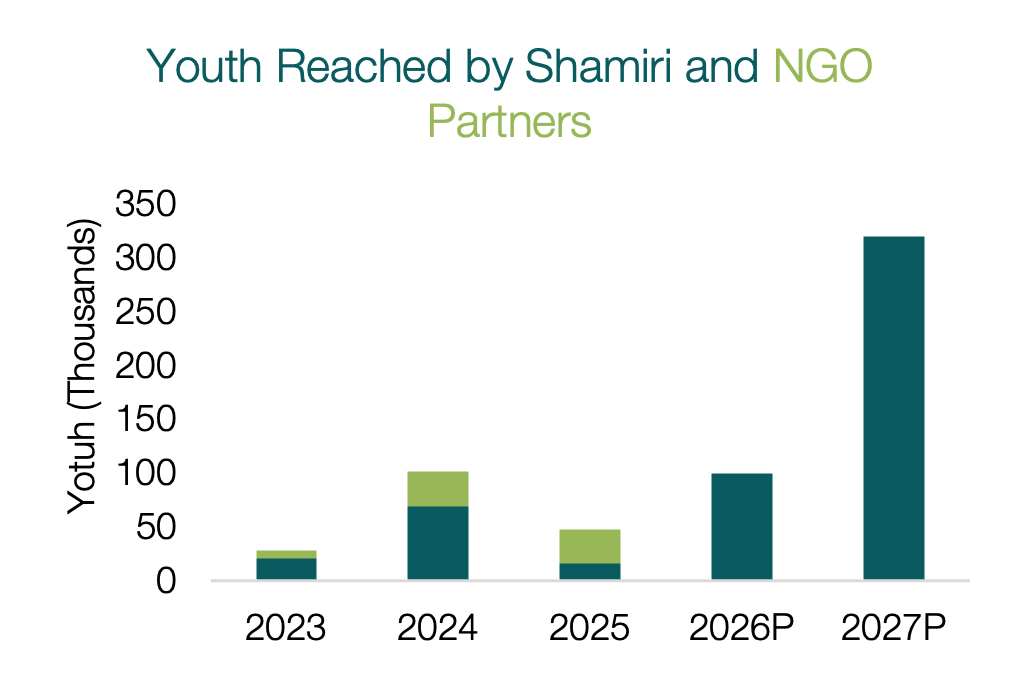
Shamiri initially was scaling through NGOs. They pivoted their scale strategy in 2026 to focus on long-term scale via government.
Impact
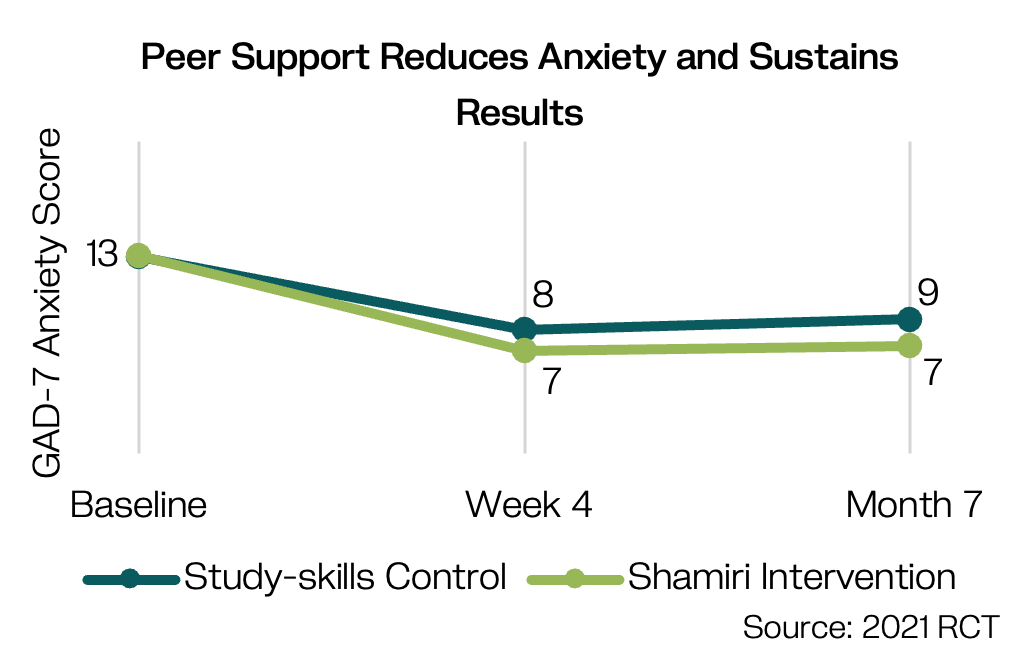
A rigorous RCT showed that Shamiri’s intervention reduces anxiety by 45% after a 7-month follow-up; the control showed a 32% decline but was not a treatment-as-usual control.
The Model
A solution that works and can scale.
Peer Providers
Recent high school graduates (ages 18–22), “Fellows”, are selected and trained to deliver sessions
Evidence-Based Curriculum
Content based on cultivating a growth mindset, gratitude, and value-aligned decision-making.
Group-Based Delivery
Four weekly 1-hour sessions, opt-in school recruitment (~80% of students sign up)
Reinforcing Homework
Take-home lessons, often done with others
Supervision and Referral
Oversight is provided by clinical supervisors; serious cases are referred
Potential for Impact at Scale
Mulago uses four criteria to gauge potential for exponential impact. The model must be:
This is about impact and evidence. In a 2021 JAMA Psychiatry RCT of 413 students (ages 13–18) with elevated symptoms in Nairobi and Kiambu, depression fell 44% at 4 weeks and 38% at 7 months; anxiety fell 48% and 45%. 80% of youth with elevated symptoms moved below the clinical threshold. The comparison group showed similar but smaller effects but was not a true control – students received study-skills sessions – so the study may understate the effect. Durability beyond 7 months and effects versus a treatment-as-usual are unknown. To scale via government, Shamiri must show school outcomes; preliminary data shows a half-letter grade improvement in academic outcomes, but more rigorous data is coming soon.
This is about scope. 50% of youth in Sub-Saharan Africa are facing mental health problems . In Kenya alone, 5M youth suffer from mental health disorders without sufficient resources or expertise to meet their needs. There’s still a lot of mental health related social stigma, but Shamiri’s curriculum is focused more on growth mindset, gratitude, and values. This relatively short weekly, 4-week intervention can be delivered in any public high school setting in Kenya. Shamiri has reached ~213K youth across 10 counties, demonstrating the model works in urban, peri-urban, and rural settings.
This is about whether the government can deliver the model. Shamiri has directly replicated their model across 10 counties in Kenya. The curriculum is straightforward and well-developed. Delivery of the curriculum depends entirely on the quality of recruited Shamiri Fellows and oversight provided by Supervisors. This part of the model has more variability and can be resource intensive (training + supervision). They’re testing what it would take for teachers and the county government to take over some of these responsibilities. This includes testing: supervisor-to-fellow ratios, tailored training approaches, and using AI to simplify and improve training and supervision.
This is about what the model costs if delivered and paid for by the government. It costs Shamiri $7/student to deliver this intervention. They are testing what price point (likely ~$3/student) and framing of the intervention makes it attractive for the Ministry of Education and parents to pay. Early willingness to pay analysis suggests most parents would pay ~$2 for mental health support for their kids. They are experimenting with two technology platforms that should drive costs down further: shamiriOS, a backend platform for streamlining operations, and shamiriAI, a tool to reduce supervisory burden while maintaining fidelity.
.png)
Shamiri is in early Growth stage, testing ways to simplify the model to enable government uptake.
Our Take
Shamiri has persuasive evidence on improving youth mental health and continues to play an important role in this sector defining a more accurate, context-specific metric for mental wellbeing. As they look to scale, they need to build evidence that matters to the Ministry of Education. To scale via government, officials and parents must see gains in school outcomes. Shamiri is collecting rigorous school outcomes data via their 2026 county pilots. The lay-provider model is promising given Africa’s shortage of psychologists and psychiatrists, but governments may struggle to recruit, train, and maintain high-quality peer providers at scale. The intervention is cheap but must get cheaper for widespreadß adoption. Shamiri is testing simpler, lower-cost delivery through streamlined training and technology-enabled models while preserving impact.
Are you a serious funder and want to learn more?
This is just a snapshot of what we know about the organization. If you're an investor or funder that might send some serious dough their way, we're always delighted to share more. Reach out and we'll connect you with the right person on our team.
*this is not monitored for funding requests.

.JPG)






