Sehat Kahani
In Pakistan, the poor do not have easy access to quality healthcare. Meanwhile, over half of Pakistan’s medical graduates are women, but only a quarter of them practice because of cultural norms.
The Idea
Telemedicine-Enabled Clinics



Total Investment
670000
Grants
0
Equity/SAFE
0
Debt/Convertible Debt
Funded Since
2020
Geography
Sector
Structure
The Mission
Healthy people in under-resourced areas.
How It Works
Sehat Kahani upgrades defunct government clinics in poor communities, staffs them with a qualified midwife or nurse, installs telemedicine capabilities, and adds a mini pharmacy for shelf-stable medications. The midwife or nurse facilitates a tele-consult between patients and a female doctor.
The Dream
Privately run, telemedicine-enabled community clinics – paid for by government – provide quality healthcare at the last mile.
Why We're In
Sehat Kahani is proving a scalable public-private model for community healthcare in Pakistan. They’ve converted 46 clinics, each serving a catchment of ~10K patients. Despite political headwinds, recent success got the attention of senior government officials. The federal government plans to roll out the model further, which is projected to dramatically increase annual consultations and signals a credible path to scale. The bet is that government will pay for the ongoing cost of delivery at these clinics.
Delivery
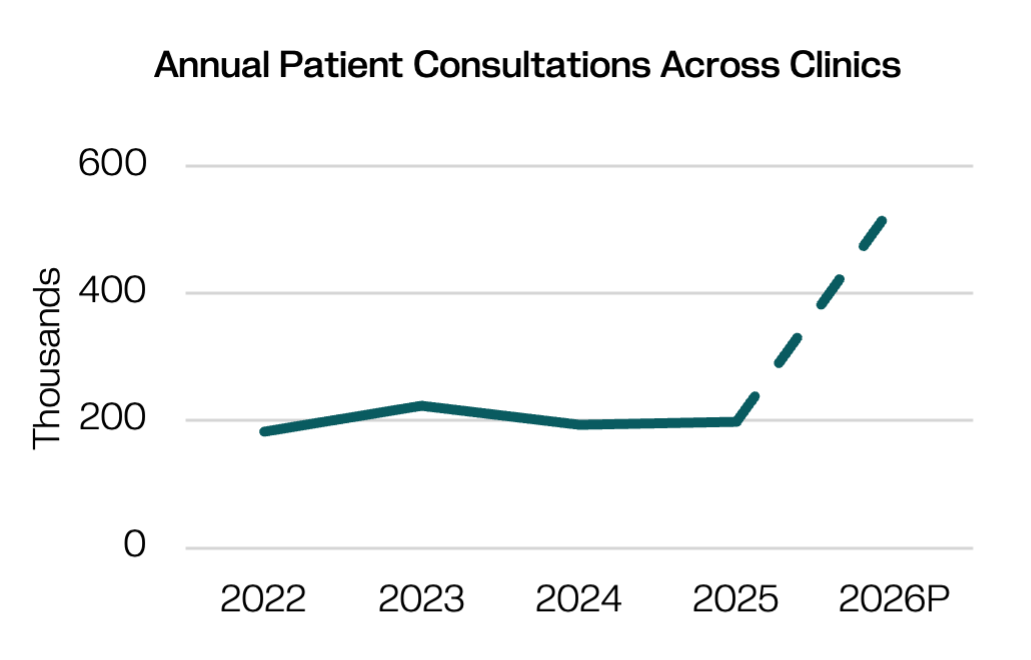
Annual patient consultations is projected to increase significantly driven by expanding government partnerships.
The Model
A solution that works and can scale.
Physical Clinic
Two-room space in communities with basic healthcare infrastructure and connectivity
Trained Providers
Qualified female health workers for clinic operations and female doctors for tele-consults
Quality Tele-Consults
Patients consult female providers over telemedicine platform
Closet Pharmacy
Shelf-stable, affordable everyday medications in-stock
Potential for Impact at Scale
Mulago uses four criteria to gauge potential for exponential impact. The model must be:
This is about impact and evidence. Sehat Kahani does not have third-party studies linking their intervention to improved health outcomes yet. However, their rigorous internal controls and quality audits adhere to the strictest standards of care that ensure consults, diagnoses, and treatment plans are high quality. Internal consultation audits show 94% accuracy rate in treatment protocols and clinical decision-making. They are designing an RCT to measure health outcomes in partnership with JPAL.
This is about scope. 100 million people in Pakistan do not have access to quality healthcare. There are ~800 defunct government-owned basic healthcare units (BHUs). Meanwhile, 70% of Pakistan’s medical graduates are female, but of these, only 23% end up being able to practice because of cultural pressure. Sehat Kahani’s model homes in on these defunct BHUs and the underutilized female physician workforce. Their model requires reliable internet connectivity and a sufficient supply of both trained in-person nurses/midwives and female doctors for tele-consults. Sehat Kahani is proving these conditions are largely in place across Pakistan.
This is about whether other businesses can replicate the model. So far, Sehat Kahani has successfully piloted the model in: Azad Jammu and Kashmir and Khyber Pakhtunkhwa (KPK). Only about 3-6% of cases cannot be treated at BHUs and require tertiary level referrals. Their successful pilots have prompted the Federal and KPK governments to explore a structured framework for contracting BHUs under a public–private partnership model. These discussions, supported by a signed MoU, aim to institutionalize a model where private providers convert and operate clinics, with government eventually covering operating costs on a per-patient basis.
This is about what the model costs if delivered by businesses and whether government is willing and able to pay. Sehat Kahani has designed an affordable model for telemedicine-enabled BHUs. Early government pilots and engagements have helped validate the operational feasibility of the model and generated momentum toward sustainable public financing pathways for long-term primary healthcare delivery through public–private partnerships.
.png)
Sehat Kahani is in early Growth stage, developing a more rigorous body of evidence and expanding to other regions after a successful public-private partnership pilot in two parts of Pakista
Our Take
Sehat Kahani has exciting momentum. While patient self-reported data on access, adherence, and health improvements is positive, this data is not yet rigorous enough. Access to affordable, quality primary healthcare is a major need across Pakistan, and Sehat Kahani is proving their model can work across a range of settings. While costs have increased significantly in the last year, they have negotiated a price structure that should still turn a significant profit margin, making this an attractive business model for others to copy. The biggest question is whether this pricing model can be sustained over time and replicated across regions with smaller budgets.
Are you a serious funder and want to learn more?
This is just a snapshot of what we know about the organization. If you're an investor or funder that might send some serious dough their way, we're always delighted to share more. Reach out and we'll connect you with the right person on our team.
*this is not monitored for funding requests.

.JPG)

.jpeg)




.png)